
If I could put one message on a billboard for anyone who smokes, it would be this:
Cigarette smoke isn’t just nicotine and tar. It’s also a delivery system for toxic metals.
And the part that really matters—especially for long-term smokers—is that some of these metals accumulate slowly, stick around for decades, and can quietly stress the body year after year.
In this article I’ll walk you through:
Let’s get into it.
Tobacco plants don’t grow in a vacuum. They grow in soil, are watered with water, are treated with fertilizers, and sit in air that can contain pollution. Tobacco also has a known tendency to accumulate cadmium—a key heavy metal we’ll talk about in a minute.
Then, when tobacco is burned, metals can be carried into smoke particles that reach the lungs. Inhalation is a particularly efficient exposure route because the lungs are designed for rapid exchange.
So, smoking becomes a repeat exposure pattern: a little metal exposure, many times, for years.
Different studies measure different metals, but the “big ones” repeatedly discussed in cigarette smoke and tobacco products include:
Cadmium and lead show up a lot in the literature as cigarette-related concerns, including studies measuring metals in cigarette brands and discussions of health risks.
If you only remember one metal from this article, make it cadmium.
Smoking is a major cadmium source
ATSDR (the U.S. Agency for Toxic Substances and Disease Registry) is very direct about this: cigarette smoke is one of the highest sources of cadmium exposure for smokers.
They also note that tobacco leaves naturally accumulate cadmium.
Smokers consistently show higher cadmium levels
Research reviews and biomonitoring-based papers repeatedly report that smokers have higher cadmium concentrations in urine, blood, hair, and tissues compared with non-smokers.
And importantly, cadmium exposure tends to correlate with pack-years (how much and how long someone smoked) and shows age-related accumulation patterns.
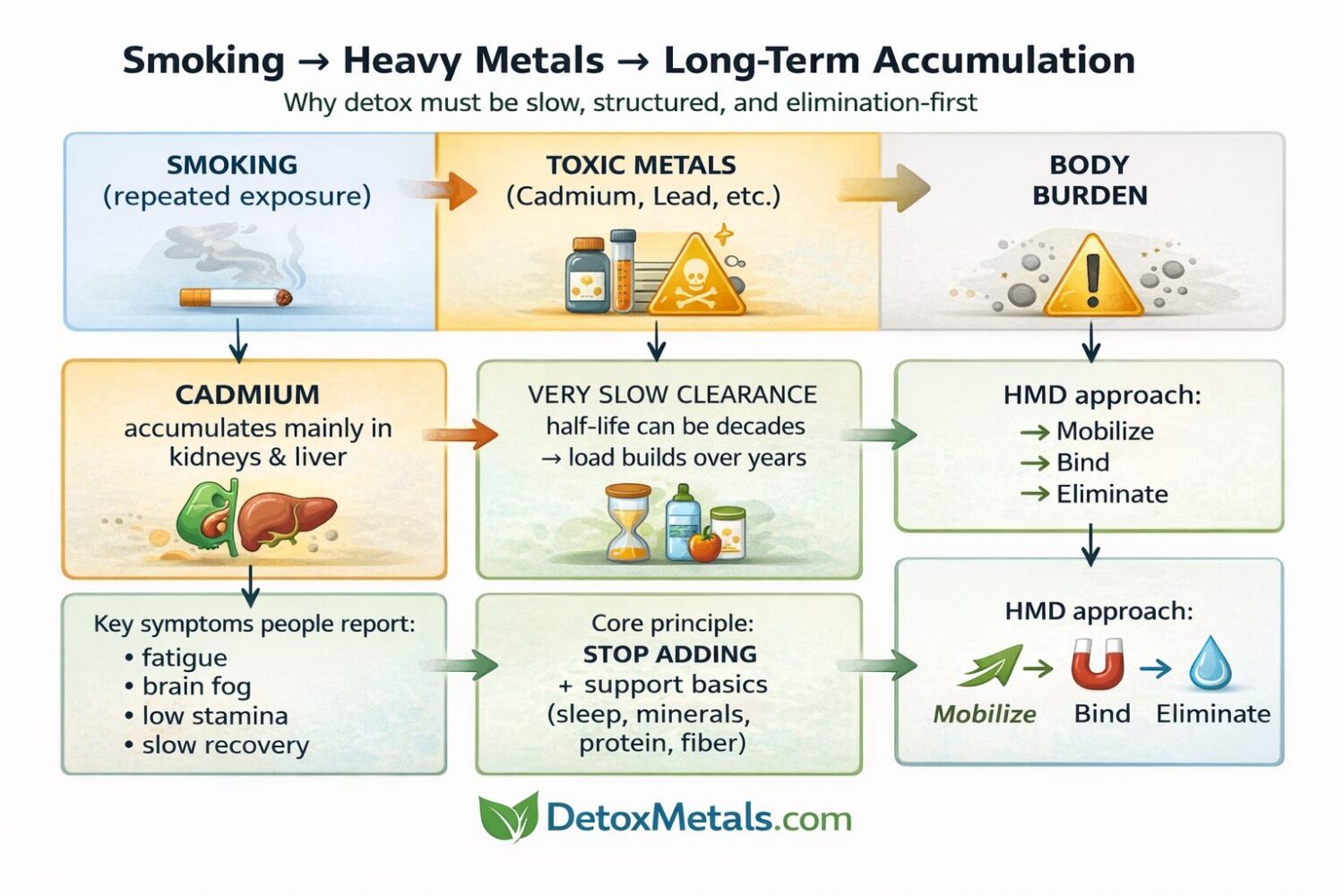
Why does cadmium accumulate long-term
Cadmium is not a metal your body “clears quickly.” ATSDR educational material describes a biologic half-life in the kidney estimated at 6–38 years (and many sources describe a long half-life in the 10–30 year range).
That means: if you smoke for decades, you’re not just dealing with “today’s cadmium.” You’re dealing with a long-term body burden that changes slowly.
Cadmium also tends to accumulate in the kidneys and liver and is slowly released, which is why urinary cadmium is often treated as a marker of longer-term exposure (with nuance).
Simple takeaway: cadmium is like a long-term house guest that doesn’t leave easily.
Lead is another heavy metal consistently linked to smoking exposure patterns.
A study examining U.S. adults found that current smokers had higher blood lead levels than non-smokers, and higher cotinine (a nicotine exposure marker) was associated with higher blood lead levels.
CDC educational content also notes that lead exposure from cigarette smoke (including second- and third-hand smoke) may contribute to increased blood lead levels in children.
Simple takeaway: smoking isn’t the only lead source in modern life, but it’s a contributor—and it can matter, especially over time and alongside other exposures.
Arsenic is also discussed in the tobacco exposure context. A WHO Europe publication notes that inhalation of arsenic (along with cadmium and benzene) is relevant for exposure in active smokers and people exposed to second-hand smoke.
And there’s emerging work on how tobacco smoke contributes to lead/cadmium/arsenic accumulating in indoor dust (third-hand smoke residue), meaning exposure can extend beyond the smoker to the home environment.
Here’s the simplest model:
1) Repeated exposure
One cigarette may deliver only small amounts of metals, but smoking is repetitive. That’s what makes it different from “one-off” exposure.
2) Inhalation is efficient
Inhalation delivers exposure through the lungs—highly vascular tissue designed for rapid transfer.
3) Some metals clear slowly (cadmium is the poster child)
Cadmium half-life measured in decades means the body burden can creep upward and only decline very slowly.
4) Stored metals can create chronic stress
Long-term metal storage can contribute to oxidative stress and inflammatory signalling—two themes that show up in many chronic disease discussions, especially in the context of smoking-related illness and cadmium exposure.
This is where it’s important to be precise. Smoking causes harm through many mechanisms (not just metals). But heavy metals are one meaningful layer of the total toxic load.
Cadmium: kidneys, bones, lungs, cardiovascular risk, cancer links
ATSDR summaries for cadmium highlight damage to kidneys, lungs, and bones.
Long-term cadmium accumulation is widely discussed as a kidney issue in particular (kidney is the main long-term accumulation organ).
Recent reviews also discuss epidemiological links between cadmium exposure and increased cancer risk across multiple sites (association-level evidence).
Lead: chronic toxicant with broad system effects
Lead is widely described as a chronic toxicant with effects on multiple systems. A UK government toxicological overview summarizes lead as a chronic toxicant and reviews its health effects across body systems.
In practical terms, lead exposure is often associated with cognitive/neurologic effects, cardiovascular issues, and more—especially with sustained exposure over time.
Brain fog is multi-factorial. For smokers, common contributors include:
So, I never tell someone, “Your brain fog is definitely metals.”
I say: metals can be part of the load, and in a long-term smoker, it’s reasonable to consider that angle.
Even if you’re not the smoker, smoke exposure can raise metal exposure.
There’s evidence linking second-hand smoke exposure to higher blood lead levels in children/adolescents, for example.
And third-hand smoke residue (nicotine and other compounds that settle and persist indoors) has been linked with metals in settled dust in some research.
Translation: smoking impacts the “micro-environment” of a home, not just the smoker.
I’m a natural health person, but I’m also a realist: the most powerful way to reduce smoking-related metal load is to stop the source.
Even cutting down frequency can help—because your body isn’t getting the same constant drip-feed of exposure.
That said, many people need a stepwise approach, and “quit” isn’t always instant. So, I think in two tracks:
That’s where detox strategy comes in.
On DetoxMetals, the core concept you’ll see repeated is:
Mobilize → Bind → Eliminate
One reason detox efforts can backfire is when people mobilize toxins (stir things up) but don’t bind and eliminate efficiently—so they feel worse.
DetoxMetals frames this clearly: “Don’t just mobilize. Bind.”
HMD® is described as a natural heavy metal detox formula developed through years of research and used clinically for many years.
The ingredient page describes a blend including Chlorella Growth Factor, Coriandrum sativum (coriander), and a homaccord of Chlorella pyrenoidosa.
And the protocol page outlines how Dr Georgiou structures detox in stages and how HMD is used within that framework.
Here’s how I explain it to patients and students:
The DetoxMetals site emphasizes binding and escorting metals toward elimination.
Smokers often carry:
So, the long-game approach matters. You’re not trying to “detox everything in a weekend.” You’re trying to support a steady, safe reduction.
This is where naturopathic common sense is everything.
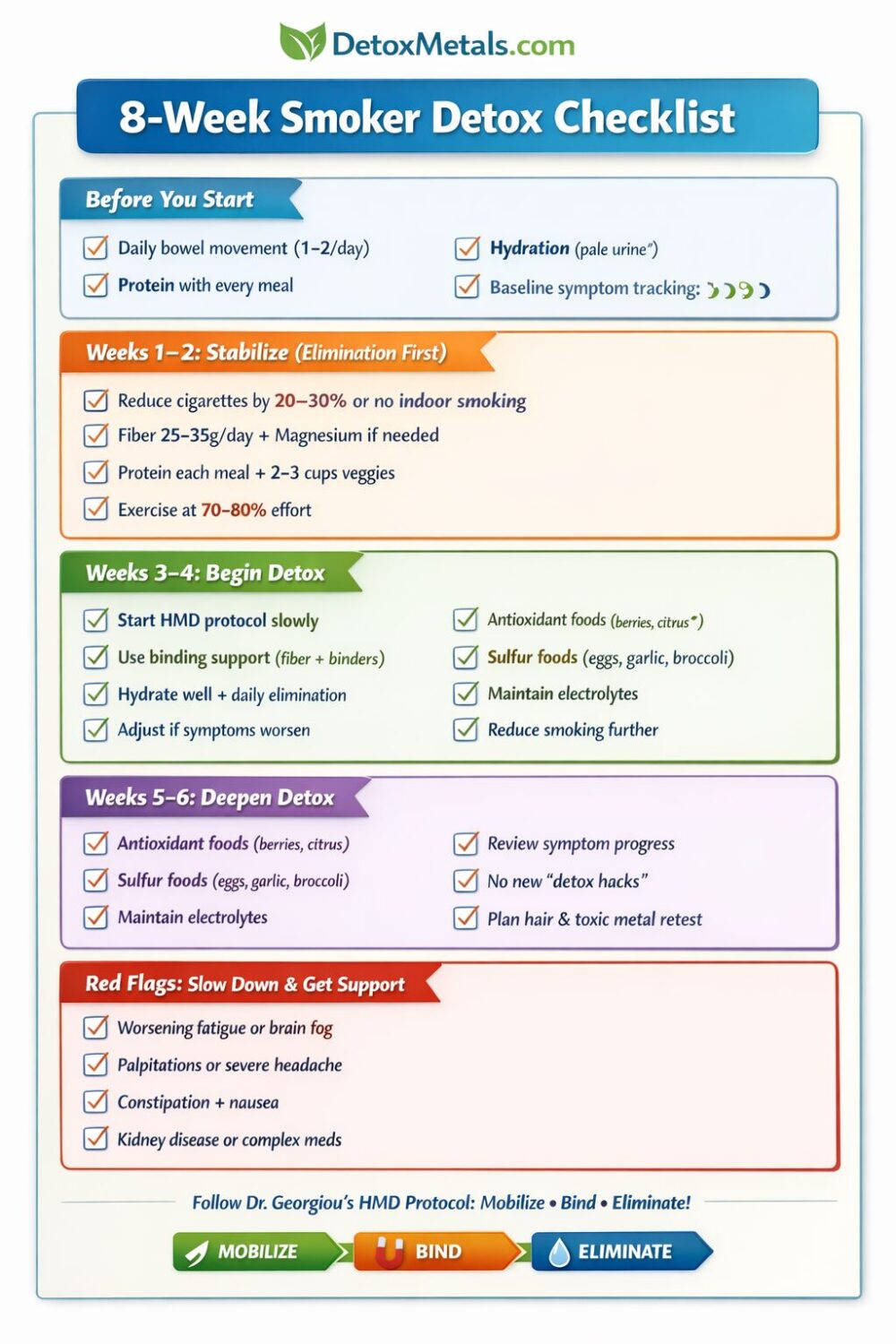
1) Prioritize elimination first (before you “push detox”)
If someone is constipated, dehydrated, or has poor bile flow, they often feel worse with detox.
Start simple:
2) Rebuild minerals (smoking is a “mineral drain” lifestyle)
Smokers commonly have higher oxidative stress and often lower nutrient reserves. Supporting minerals isn’t “optional”; it’s part of resilience.
3) Go slower than your ego wants
Long-term cadmium burden isn’t a quick fix.
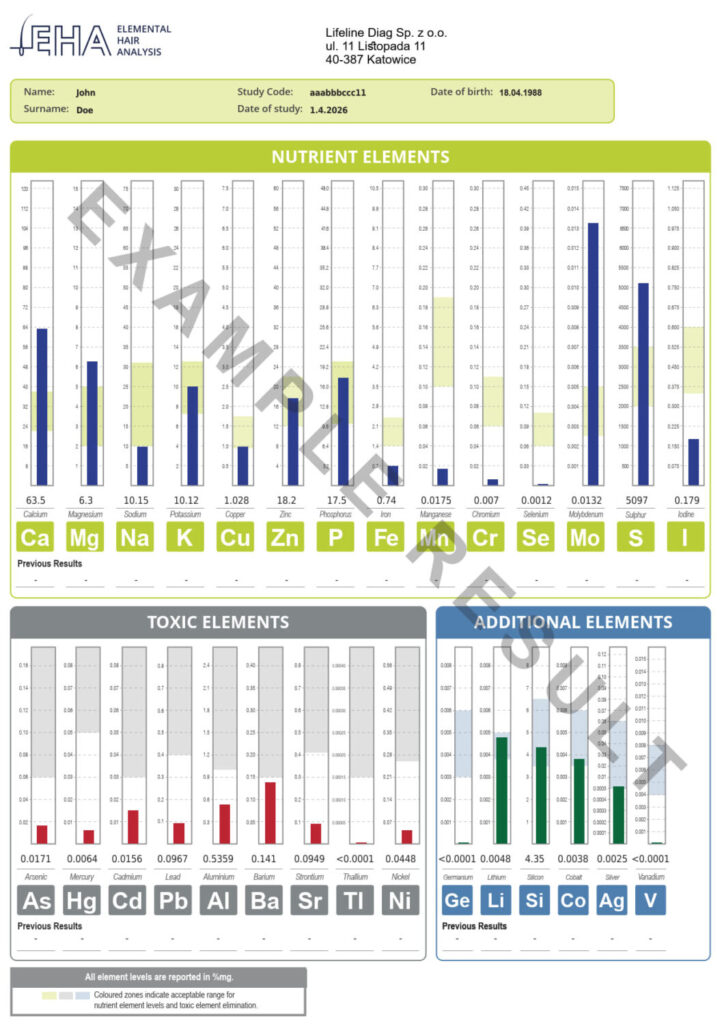
4) Track progress with testing (pattern + trend)
DetoxMetals often recommends a baseline approach with retesting to track trends (for example, using HTMA/hair testing as a clinical decision tool).
For a smoker, tracking matters because symptoms are vague and life is noisy—data helps.
I’ll keep this grounded: not everyone has dramatic changes, and results depend on the full picture (sleep, stress, diet, gut function, thyroid, etc.). But clinically, the symptom clusters people commonly hope to improve include:
If the main driver is still active smoking, improvements may be limited—again, the source matters most.
Step 1: Reduce exposure
Step 2: Assess symptoms and risk
Use a symptom questionnaire and consider whether fatigue/brain fog/recovery issues fit a “toxic load” pattern.
Step 3: Consider testing
If you want objective data, hair mineral analysis can be used as a pattern/trend assessment tool (especially combined with mineral status).
Step 4: Follow a structured protocol
Use a gradual Mobilize → Bind → Eliminate approach as described in Dr Georgiou’s protocol and supporting pages.
Step 5: Retest and refine
Detox is not a one-and-done event—it’s a process. Re-testing helps you evaluate whether the plan is moving the needle.
Smoking is a well-documented source of toxic metal exposure, especially cadmium, with evidence showing higher cadmium biomarkers in smokers and a biologic half-life measured in decades.
Smoking is also associated with higher blood lead levels in population studies.
Over years, this becomes part of the chronic load that can contribute to fatigue, inflammation, and long-term health risks—on top of all the other harms of smoking.
And that’s why, in my view, a smart approach combines:





PODCAST: HEAVY METALS IN A MODERN LIFESTYLE Heavy Metals in a Modern Lifestyle The New Detox Problem How everyday food, air, water, products and technology may be adding to our

PODCAST: Wildfire Smoke, Toxic Ash, and Heavy Metals in Our Air Wildfire Smoke, Toxic Ash and Heavy Metals The Hidden Side of Air Pollution Wildfire smoke is no longer

The Heavy Metal Problem in “Healthy” Foods Most people trying to improve their health start in the same place: they clean up their diet. They cut back on processed foods,





