






HEAVY METALS & LIFESTYLE
Heavy Metals Are Still a Modern Health Problem
Heavy Metals: A Silent Threat to Modern Health And What to Do About It A lot of people still think heavy metal toxicity is an old-world problem — something tied

Aluminium is not usually the first metal people think about when they hear the word “neurotoxicity.” Yet it is one of the most common metals in our environment, and human exposure is routine. It reaches us through food, food additives, food packaging, drinking water, medications, and industrial sources.
On top of that, nano-sized aluminium and alumina particles are now a growing toxicology concern because particles at that scale can behave differently from ordinary bulk aluminium.
A recent 2025 review on aluminium nanoparticles described the brain as one of the primary target organs in animal studies, while a 2026 review on aluminium oxide nanoparticles said their small size allows them to cross biological barriers and accumulate in the central nervous system.
That does not mean we can honestly say nano-aluminium is a proven sole cause of Alzheimer’s disease in humans. We cannot. The human evidence is still debated. But the scientific case that aluminium is a neurotoxic metal is strong, and the case that it may contribute to Alzheimer’s-type pathology is much more serious than many people realize.
Recent reviews continue to describe aluminium-induced neurotoxicity as biologically plausible in Alzheimer’s disease, while also acknowledging that direct causality in humans remains unsettled.
The “nano” part matters. Nanoparticles have a much larger surface area relative to their size, which often makes them more chemically reactive and potentially more biologically disruptive than the same substance in larger form.
EFSA notes that nanomaterials can show different physical and chemical properties from the same materials at conventional scale. More broadly, nanotoxicology research has shown that nanoscale materials can reach the brain via the blood-brain barrier or even the nose-to-brain olfactory route, and that oxidative stress and inflammation are central mechanisms of damage.
That matters because aluminium exposure is already widespread in daily life. EFSA has long identified the diet as the major source of aluminium exposure for the general population, with food additives and food-contact materials contributing to that load, while WHO continues to include aluminium in its drinking-water guideline framework.
StatPearls likewise notes exposure from food packaging, food additives, drinking water, medications, and industrial sources. Separately, the food sector is increasingly using metal and metal-oxide nanoparticles in processing and packaging, which creates an oral exposure question that toxicologists are taking seriously.
So the realistic picture is this: ordinary aluminium exposure from food and water is already common, and nano-sized aluminium or alumina particles add a newer layer of concern, especially because small particles can stay suspended in water systems and show different toxicokinetics.
A 2024 freshwater study on alumina nanoparticles specifically noted that these particles can remain suspended in water for extended periods, which is one reason environmental exposure is being watched more closely.
The epidemiology is mixed, and that is important to say plainly. Some drinking-water studies have found little or no association at lower exposure levels, while others have reported higher Alzheimer’s or dementia risk in areas with higher aluminium concentrations.
For example, a large French cohort found roughly a doubling of dementia risk above 0.1 mg/L aluminium in drinking water, while a 2021 Canadian cohort did not find a clear overall association, although it did see a positive trend in the ApoE-ε4 genetic subgroup. In other words, the human evidence is not neat or uniform.
But epidemiology is only one part of the story. Mechanistic studies increasingly show that aluminium can trigger several of the same biological changes that define Alzheimer’s disease: amyloid-beta buildup, tau hyperphosphorylation, neuroinflammation, oxidative stress, mitochondrial dysfunction, and breakdown in cellular cleanup systems like autophagy.
That is why this topic continues to come back. Even when population data are inconsistent, the biology keeps pointing in the same direction.
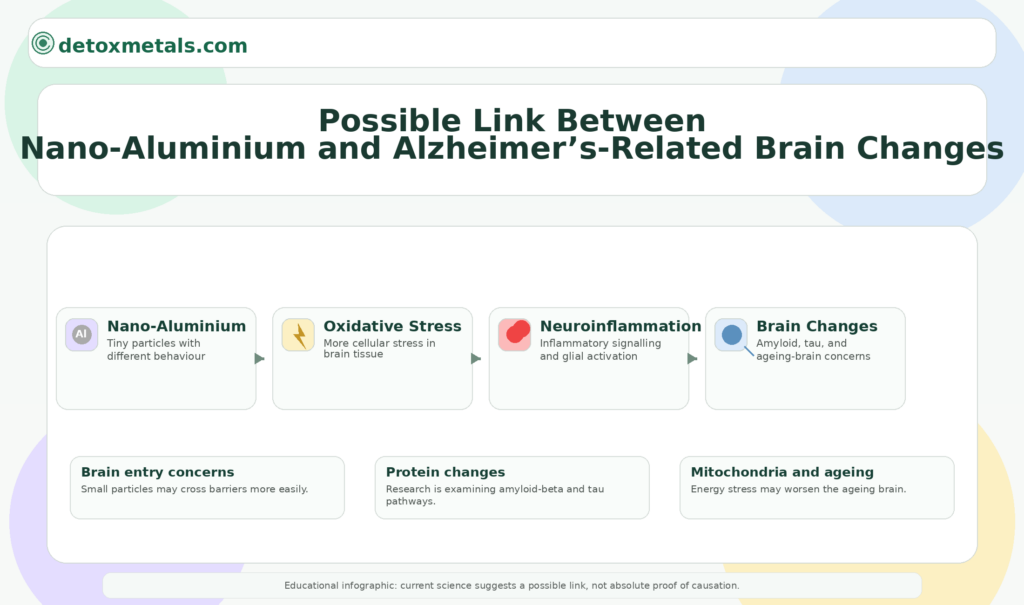
One of the biggest worries with nano-aluminium is that smaller particles can gain access to the brain more easily than larger particles. The newer 2026 review on aluminium oxide nanoparticles specifically states that their size allows them to cross biological barriers and accumulate in the CNS, while the broader nanoneurotoxicity literature describes both blood-brain barrier passage and olfactory transport as plausible routes into the brain.
Once there, the particles may directly injure neurons or act indirectly through glial activation and inflammatory signaling.
This matters for Alzheimer’s disease because the illness begins years before symptoms appear. Anything that increases brain exposure to a reactive, non-essential metal is relevant to long-term neurodegeneration.
A recurring theme in aluminium toxicology is oxidative stress. The 2025 review on aluminium nanoparticles says that much of their toxicity appears to involve oxidative stress, mitochondrial dysfunction, inflammation, genotoxicity, and cell death pathways.
The broader aluminium toxicity literature says much the same. In the brain, oxidative stress is especially damaging because neurons are energy-hungry, long-lived, and relatively poor at replacing themselves. Alzheimer’s disease is already strongly linked with oxidative damage and mitochondrial failure, so aluminium may be acting like an accelerant on processes the Alzheimer’s brain is already vulnerable to.
Another major mechanism is neuroinflammation. A 2023 experimental paper found that aluminium activated microglia and drove inflammation through the P2X7–NLRP3 inflammasome pathway, increasing inflammatory cytokines and worsening neuronal injury.
This is important because chronic microglial activation is now seen as a major part of Alzheimer’s progression, not just a side effect. If aluminium is helping switch on those inflammatory circuits, it may be pushing the brain toward an Alzheimer’s-like state even before major cognitive decline is obvious.
This is the mechanism most people associate with Alzheimer’s, and aluminium is repeatedly implicated here. A 2023 review on aluminium neurotoxicity and autophagy notes that aluminium exposure is believed to influence amyloid-beta production and tau hyperphosphorylation, two of the central pathologies in Alzheimer’s disease.
A 2021 study also found that aluminium, particularly in the presence of ApoE-ε4, increased tau phosphorylation and Aβ deposition, while another human tissue study reported aluminium co-localized with phosphorylated tau in familial Alzheimer’s disease brain tissue. These findings do not prove aluminium started the disease, but they show a close relationship between aluminium and the exact lesions Alzheimer’s is known for.
Healthy neurons rely on autophagy to clear damaged proteins and organelles. When autophagy breaks down, proteins like amyloid-beta and tau can accumulate. The 2023 autophagy review argues that dysfunction of this cleanup system may be one way aluminium worsens neurotoxicity and allows toxic proteins to build up. In simple terms, aluminium may not only increase the production of bad proteins; it may also weaken the brain’s ability to clear them away.
A newer and more cutting-edge mechanism involves epigenetics. A 2024 review focusing on aluminium-induced neurotoxicity and Alzheimer’s disease reported that aluminium exposure can disturb DNA methylation, histone modification, and microRNA expression.
Those epigenetic changes were linked to increased APP and BACE1 expression, heightened NF-κB inflammatory signaling, and other shifts that could favor Alzheimer’s-type pathology. This is important because it suggests aluminium may leave a deeper molecular imprint than simple one-time toxicity.
I think the fair conclusion is this: the human evidence is not definitive enough to say nano-aluminium alone “causes” Alzheimer’s disease in every case, but there is now a strong and growing mechanistic case that aluminium — especially in more bioavailable or nano-sized forms — can contribute to the biology of Alzheimer’s disease.
The strongest evidence sits in the overlap between brain entry, oxidative stress, inflammation, amyloid/tau pathology, autophagy failure, and epigenetic change. That is a serious cluster, not a minor footnote.
And this is why reducing overall toxic-metal burden makes sense even before absolute scientific certainty arrives. Alzheimer’s disease is multifactorial. Metals do not need to be the only cause to still be an important and modifiable contributor.
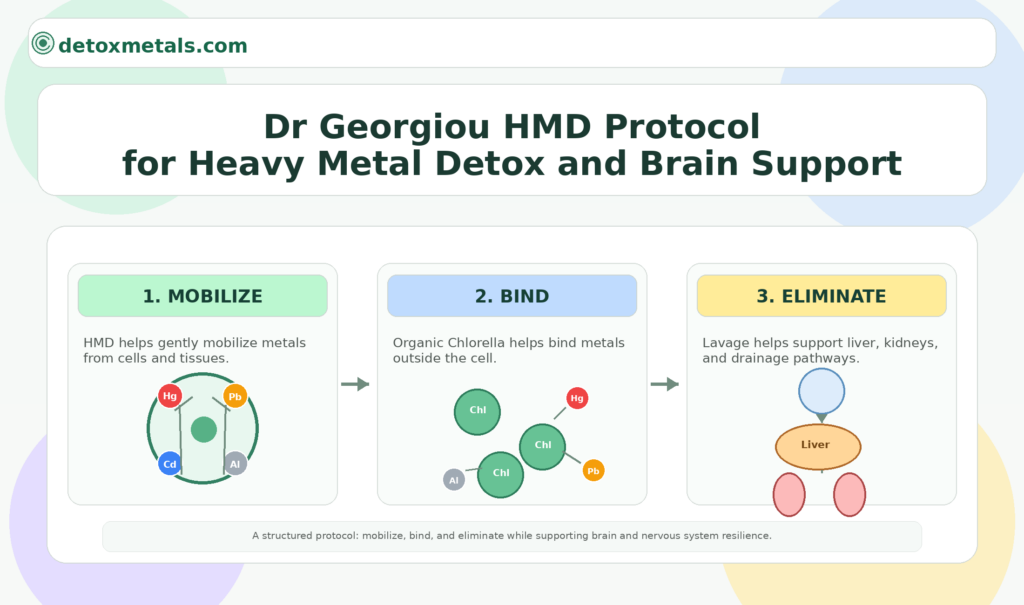
If aluminium and other toxic metals are part of the long-term neurodegenerative burden, the next question is obvious: what can be done about it? This is where Dr Georgiou’s HMD protocol is worth mentioning. According to Detox Metals, the protocol is built as a three-part system rather than a single detox product.
HMD® is the mobilizing component that helps “pull” metals from inside the cell, HMD® Organic Chlorella helps bind metals outside the cell, and HMD® Lavage is the drainage support intended to help upregulate the detoxification pathways of the liver, kidneys, and lymphatics while supporting elimination.
The current adult guidance published on the protocol page is HMD® 45 drops three times daily, HMD® Lavage 25 drops three times daily, and HMD® Organic Chlorella 2 capsules twice daily with meals.
Detox Metals presents this as a coordinated protocol because mobilizing metals without binding and drainage support risks redistribution rather than proper elimination.
That does not make HMD an Alzheimer’s treatment, and I would not present it that way. But for readers concerned about aluminium and other toxic metals as part of long-term brain-health risk, Dr Georgiou’s protocol offers a structured detox framework built around mobilization, binding, and elimination — which is a more biologically sensible approach than a random quick cleanse.





Heavy Metals: A Silent Threat to Modern Health And What to Do About It A lot of people still think heavy metal toxicity is an old-world problem — something tied

A major 2025 study found that 14–17% of the world’s cropland may be contaminated with toxic metals. Here’s what that means for your food and your health. Heavy Metals
A Conversation on Inner Detox Today I want to speak about a different kind of healing. Many people know Dr. Georgiou for his work in the field of physical detox